The Number of LDL Particles: The Hidden Metric That Explains True Atherosclerotic Risk in Dyslipidemia
LDL-C as a Traditional Therapeutic Target
Historically, LDL-C has been maintained as the primary therapeutic target in the prevention of atherosclerotic cardiovascular disease (ASCVD), with the goal of reducing its plasma concentration as much as possible. However, the prevalence of residual risk—even in patients with LDL-C levels within the optimal range—has compelled the scientific community to seek more precise biomarkers.
Figure 1.
The Liposcale Test® and Advanced Lipoprotein Analysis
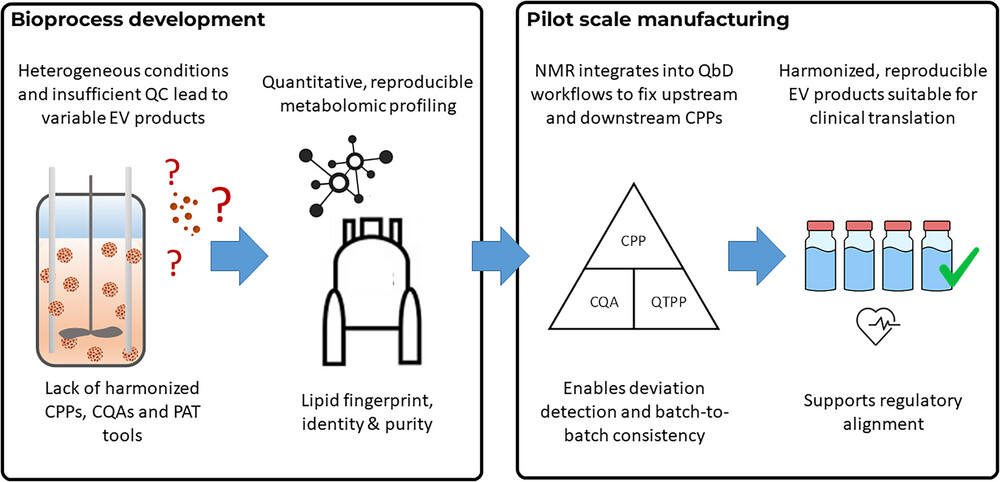
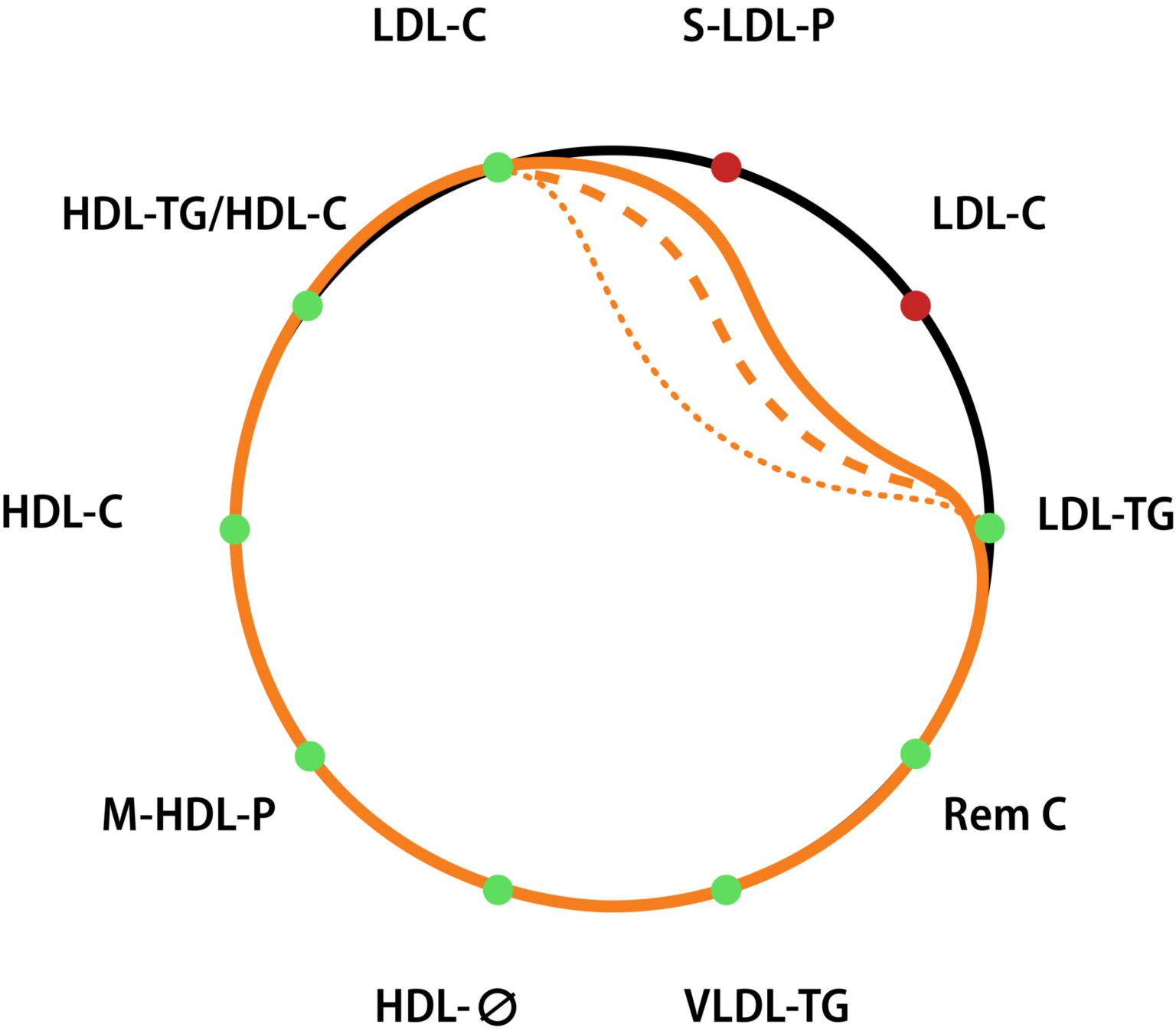
The Liposcale Test® addresses this need by offering advanced lipoprotein analysis based on Nuclear Magnetic Resonance (NMR) spectroscopy. NMR enables the direct determination of particle concentration (LDL-P), size (diameter), and lipoprotein composition. The reason these parameters are superior to LDL-C lies in the underlying physics of cholesterol transport and the atherogenic process.
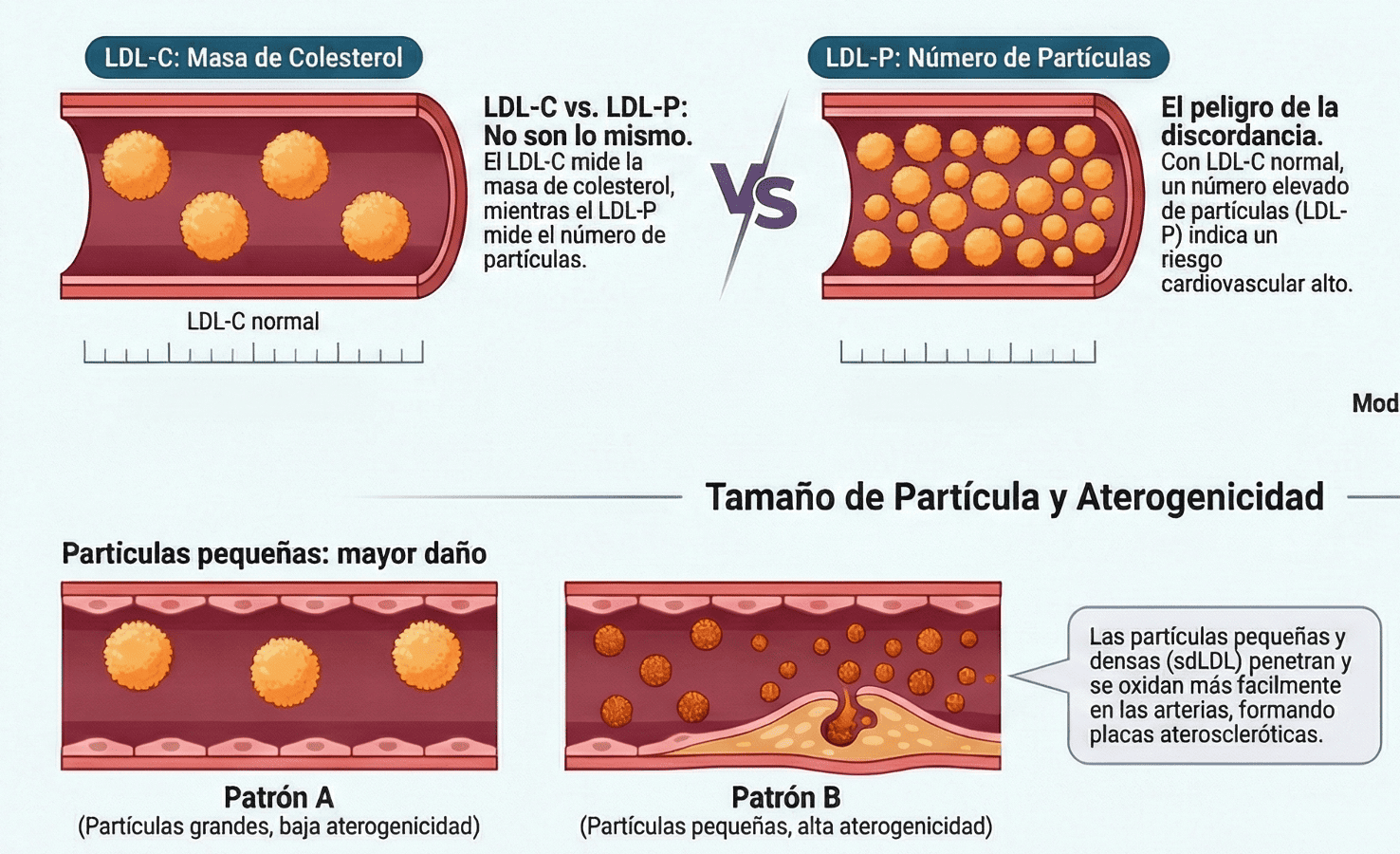
The atherogenic potential of a lipoprotein is determined by its number, size, and composition. Each LDL particle contains a single molecule of Apolipoprotein B (ApoB), making the measurement of particle number (LDL-P) a more direct and precise indicator of the total number of atherogenic lipoproteins circulating in the blood. In contrast, LDL-C only measures the total amount of cholesterol contained within those particles, ignoring their total number.
LDL-C:LDL-P Discordance in Atherogenic Dyslipidemia
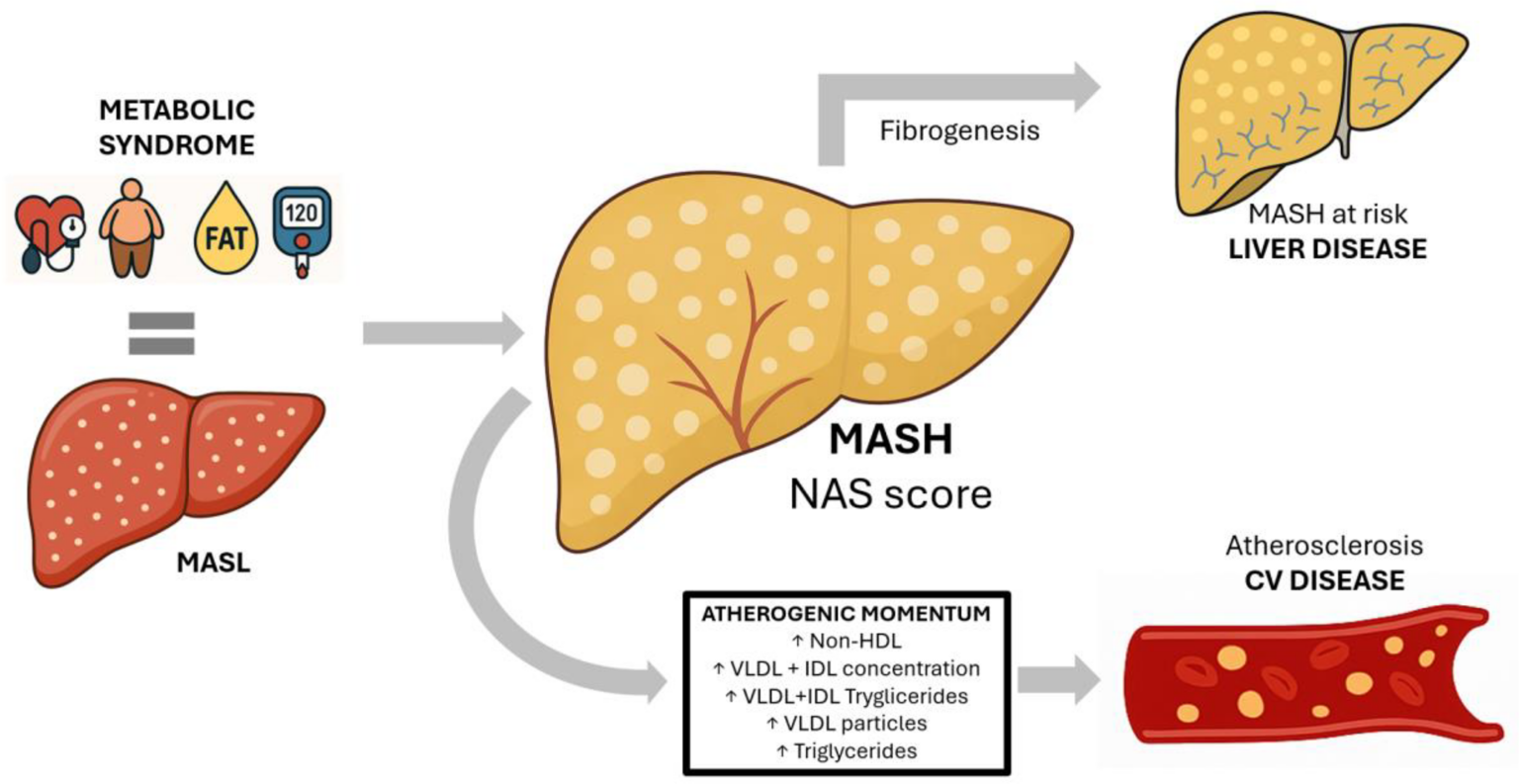
In the context of atherogenic dyslipidemia (AD), common in diabetes mellitus (DM) and metabolic syndrome, LDL-P concentration may be clearly elevated even when LDL-C is normal or only mildly increased. This LDL-C:LDL-P discordance is crucial, as a normal LDL-C with a high particle number implies that these particles are predominantly small and dense LDL (sdLDL).
Reasons for the High Atherogenic Potential of sdLDL
sdLDL particles have high atherogenic potential for several reasons:
Greater arterial retention: Smaller LDL particles penetrate the arterial wall in greater numbers and undergo increased retention and modification in the intima, the primary event in atherogenesis.
Greater susceptibility to oxidation: sdLDL particles are more susceptible to oxidation, and LDL oxidation is a key step in the development of atherosclerotic plaque.
Lower affinity for the LDL receptor: sdLDL particles have reduced affinity for the LDL receptor, contributing to their longer residence time in circulation
Epidemiological Evidence and Predictive Value of LDL-P
Large-scale epidemiological studies have shown that LDL-P better predicts cardiovascular events than LDL-C. For example, in the Framingham Offspring Study, LDL-P concentration proved to be a more sensitive indicator of cardiovascular disease (CVD) risk. Furthermore, NMR subclass analysis has shown that medium-sized LDL particles are positively associated with cardiovascular, coronary, and cerebrovascular events.
Clinical Application of Liposcale® in High-Risk Populations
The Liposcale® test allows clinicians to identify atherogenic dyslipidemia in high-risk populations such as those with diabetes, obesity, metabolic syndrome, or hypertriglyceridemia. By quantifying LDL-P and determining whether the profile is skewed toward a predominance of small, dense LDL particles, the test helps avoid underestimation of cardiovascular risk (CVR). This is crucial for therapeutic decision-making and prevention strategies, even when LDL-C is at target levels.
In fact, increased LDL-P has been associated with myocardial infarction, ischemic stroke, and peripheral arterial disease. Evidence suggests that therapeutic monitoring based on LDL-P allows for better assessment of residual risk.
The linked resource provides an external overview of payment rails, processing times and accepted withdrawal methods at Australian-facing online casinos, including POLi, PayID, various e‑wallet providers and crypto options; it can help readers compare typical processing speeds, minimum withdrawal limits, and fee practices across platforms and check whether a site lists auditing or licensing details. https://winterblueschampionship.com/highest-paying-online-casino-australia/ It is presented here solely as a separate informational reference for those wanting more granular payment and withdrawal information.