Cardiovascular diseases remain the leading cause of death worldwide.
Despite preventive efforts—such as controlling LDL cholesterol, blood pressure, and glucose levels—many individuals still suffer heart attacks or strokes even with apparently “normal” values.
This phenomenon is known as residual cardiovascular risk, and it accounts for up to 60–70% of cases. A study published in the American Heart Journal in 2009, based on more than 130,000 patients hospitalized for coronary artery disease, showed that over 50% had optimal LDL cholesterol levels at the time of admission. This finding highlights that LDL cholesterol alone is not a sufficient indicator of cardiovascular risk (1).
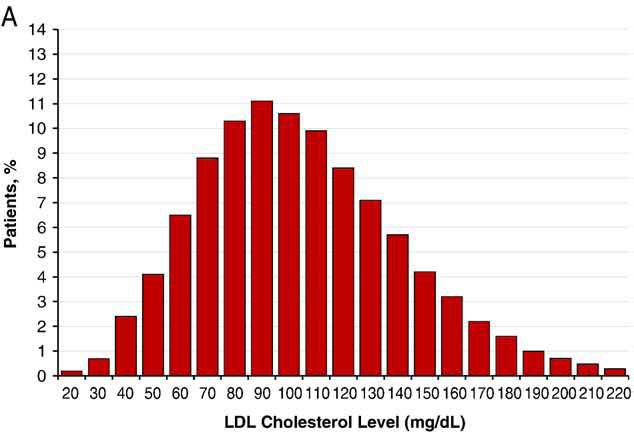
Figure 1: Histogram of LDL levels at admission in 10 mg/dL increments.
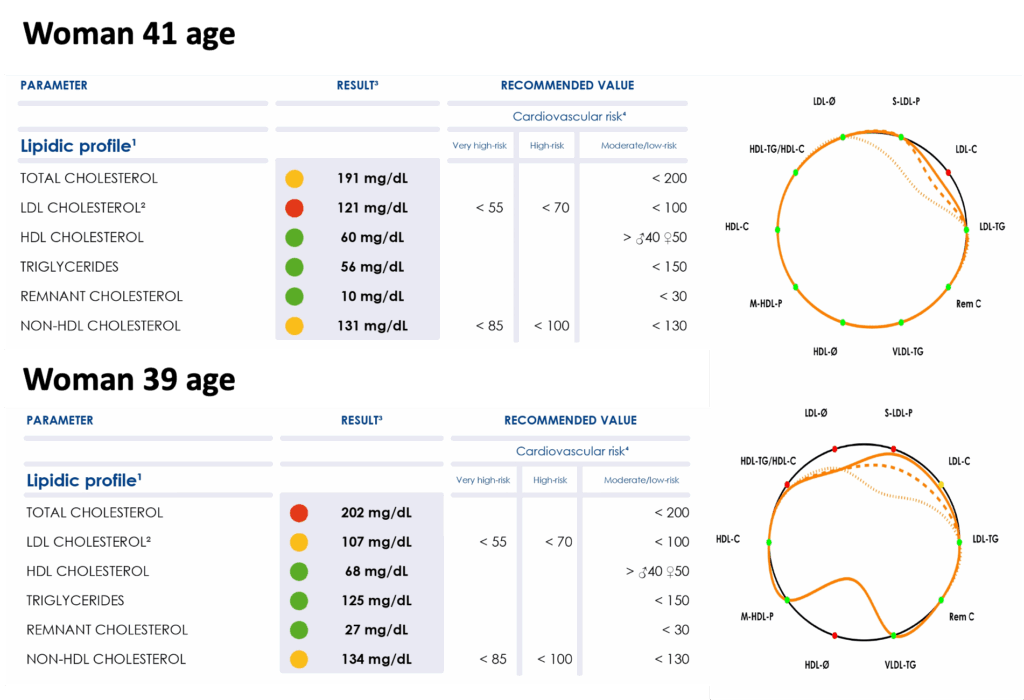
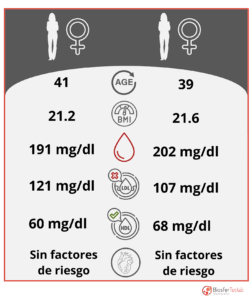 We present the case of two women of similar age (41 and 39 years), with no known risk factors and a normal body mass index (21.2 and 21.6 kg/m², respectively). Both have appropriate levels of total cholesterol, LDL, and HDL. At first glance, their cardiovascular profiles appear healthy.
We present the case of two women of similar age (41 and 39 years), with no known risk factors and a normal body mass index (21.2 and 21.6 kg/m², respectively). Both have appropriate levels of total cholesterol, LDL, and HDL. At first glance, their cardiovascular profiles appear healthy.
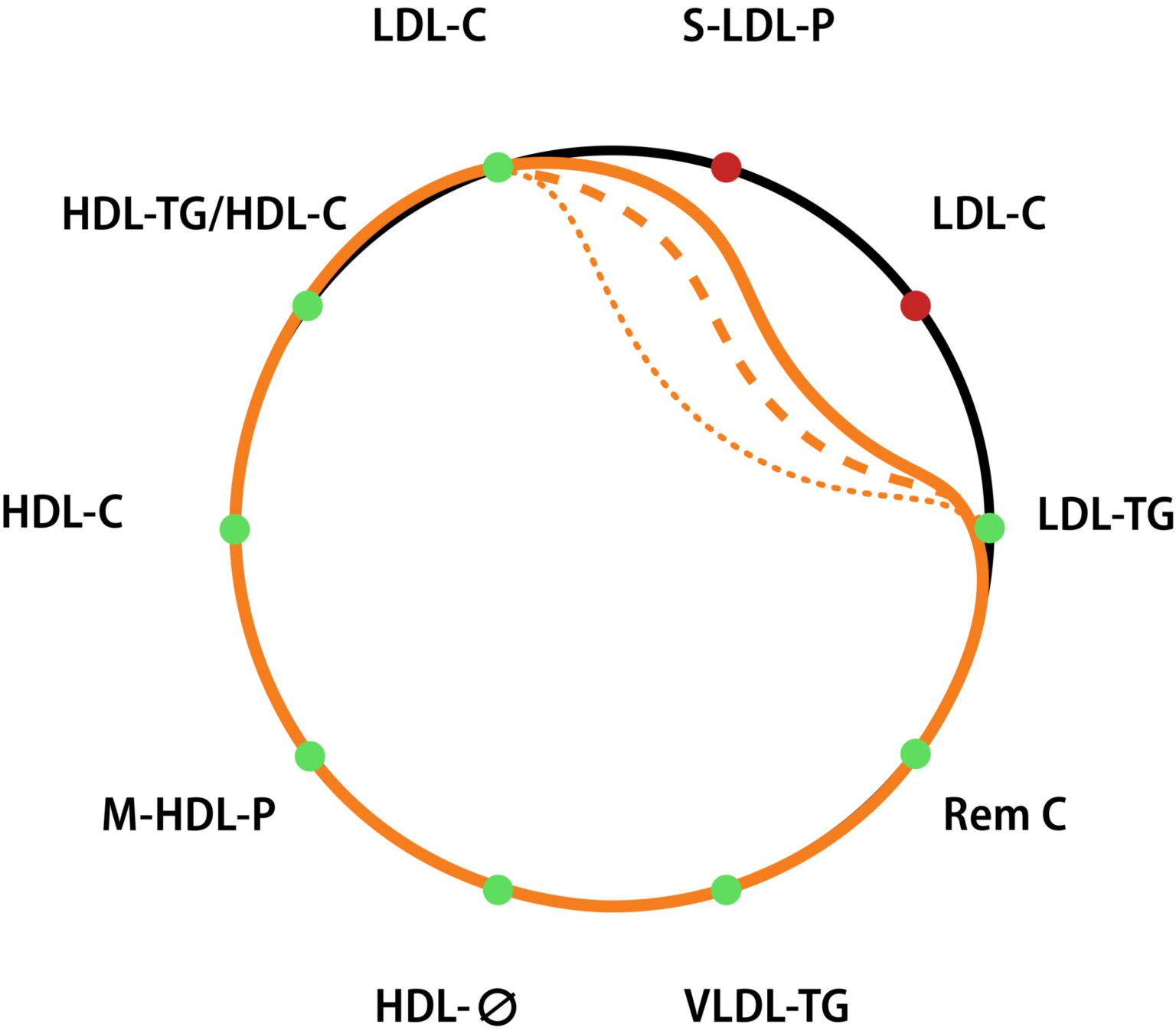
However, when both women underwent evaluation using the Liposcale® test, the results told a different story. Although their standard lipid profiles (Figure 3, left) appear quite similar, a more detailed analysis of their lipid profiles (Figure 3, right) reveals significant differences. Interestingly, the woman with the lower LDL cholesterol levels shows more pronounced alterations in her lipoprotein profile, which is clearly reflected in her lipid signature.
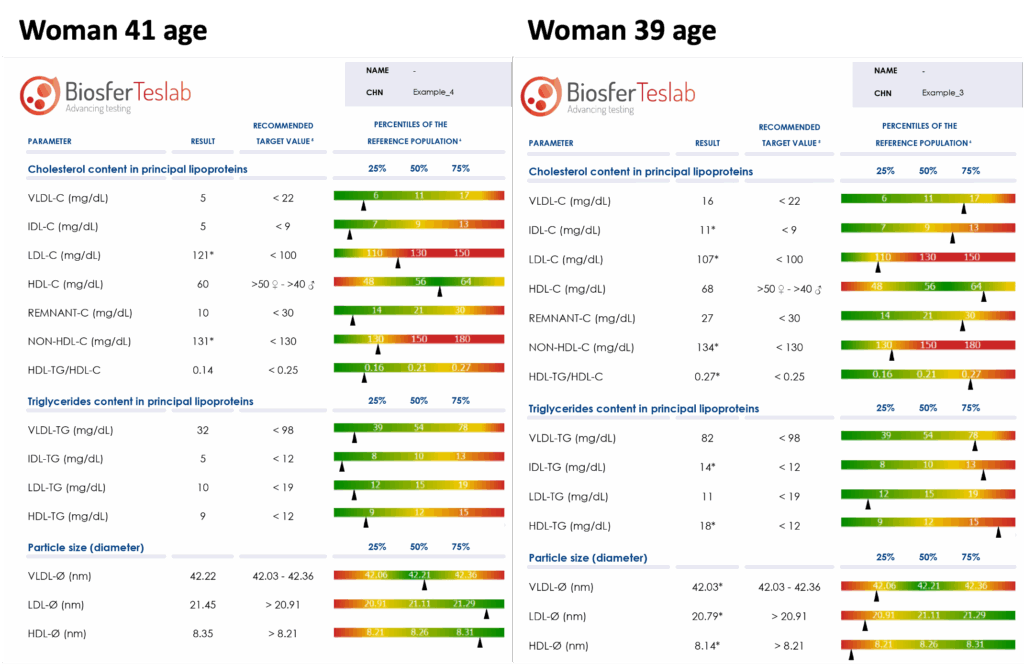
A closer look at a portion of the comprehensive lipid panel provided by the Liposcale® test (Figure 4) shows that, while both women present fairly similar values, one tends to fall within the green range, whereas the other displays more values in the yellow range. This suggests that, despite having seemingly normal values in conventional parameters, the latter has a more pro-atherogenic profile and therefore a higher cardiovascular risk, even in the absence of traditional risk factors. Moreover, the analysis of the mean particle size further supports this pattern, once again indicating a more pro-atherogenic profile in her case.