Triglycerides: More Than a Marker — A Driver of Cardiovascular Risk
Triglycerides: More Than a Marker — A Driver of Cardiovascular Risk
Introduction: The Residual Risk Beyond LDL Cholesterol
For decades, LDL cholesterol has been considered the main enemy in cardiovascular prevention. However, numerous studies — including the FOURIER-OLE trial — have shown that even patients with extremely low LDL-C levels continue to experience cardiovascular events. This phenomenon is known as residual cardiovascular risk.
Among the contributing factors, triglycerides (TG) and triglyceride-rich lipoproteins (TRLs) stand out as key players. These particles, which include VLDL and their remnants, are highly atherogenic, and their excess reflects a global disturbance of lipid metabolism.
Study Aim: Visualizing Global Lipid Alterations
The study, published by Núria Amigó, Pol Torné, Liv T. Nordestgaard, Francesco Di Giacomo-Barbagallo, Carla Merino, Paolo Magni, Ana González-Lleó, Natalia Andreychuk, Alberico L. Catapano, Lluís Masana, and Daiana Ibarretxe, investigated how rising triglyceride levels modify the entire lipoprotein profile.
The research team used nuclear magnetic resonance (¹H-NMR) spectroscopy — via the Liposcale® method — in 822 patients with metabolic alterations followed at a specialized hospital lipid unit.
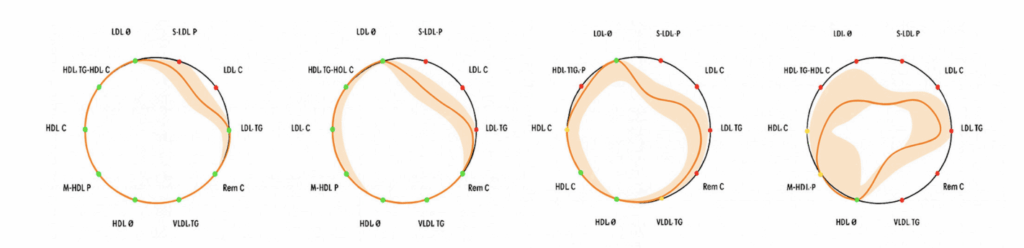
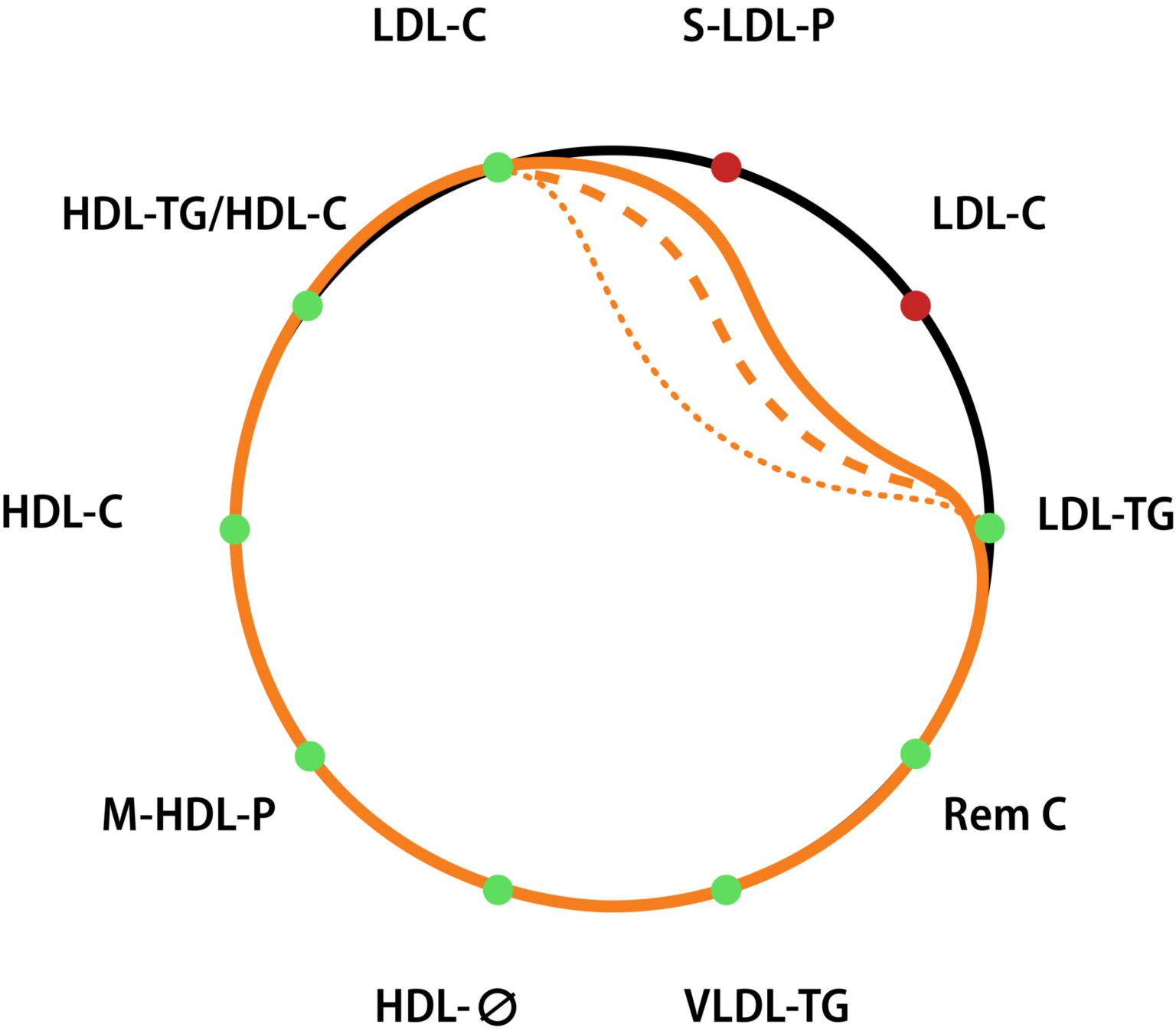
In addition, they developed an innovative visualization tool called the “Lipid Silhouette” (LS), a circular graphical representation summarizing ten key lipoprotein parameters, allowing clinicians to instantly visualize how higher TG levels distort the patient’s lipid balance.
Main Findings: A Progressive Lipoprotein Derangement
Participants were divided into triglyceride quartiles, from normal values (<1.05 mmol/L) to hypertriglyceridemia (>2.17 mmol/L). The results were striking:
VLDL particles increased up to six-fold in the highest quartile, especially the smaller, more atherogenic ones.
Remnant cholesterol — cholesterol carried by VLDL and IDL — quadrupled, accounting for up to 30% of total cholesterol in patients with the highest TG levels.
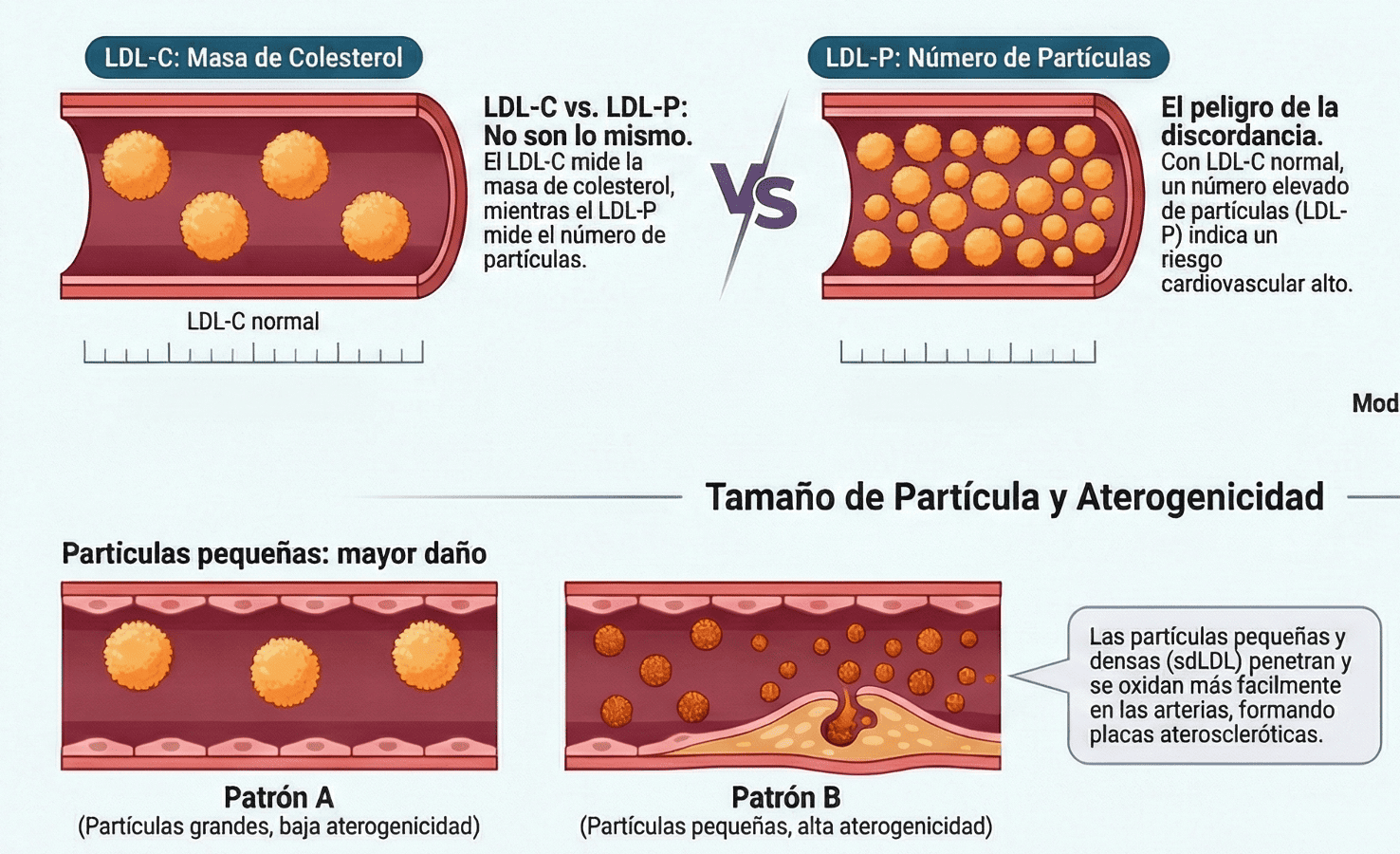
LDL particles became smaller and denser, with a 50% rise in small LDL, known for their greater arterial penetration.
HDL particles, traditionally protective, decreased in number and became enriched in triglycerides, reducing their functionality. The HDL-TG/HDL-C ratio more than doubled.
Together, these changes define a global pro-atherogenic lipoprotein profile, clearly visible through the lipid silhouette, which progressively contracts as triglyceride levels rise.
Figure 1. Mean lipid silhouettes derived from ten lipoprotein parameters measured by nuclear magnetic resonance (1H–NMR) in patients categorized by triglyceride concentration quartiles. Al- teration of parameters are represented as a contraction of the silhouette towards its center, with the extent of contraction proportional to the variance of the respective parameter. LDL–Z: LDL diameter size; S–LDL–P: smaller LDL particles; LDL–C: LDL cholesterol; LDL–TG: LDL triglyc- erides; Rem C: Remnant cholesterol; VLDL–TG: VLDL triglycerides; HDL–Z: HDL diameter size; M–HDL–P: number of medium-size HDL particles; HDL–C: HDL cholesterol; HDL–TG/HDL–C: HDL triglycerides/cholesterol ratio. The shadow represents the confidence interval.
Table 1. Baseline clinical and biochemical characteristics of the studied population categorized by the absence or presence of diabetes and obesity (D/O) and further stratified into tertiles according to serum triglyceride concentrations (mmol/L).
Independent of Obesity or Diabetes
Although obesity and type 2 diabetes often accompany hypertriglyceridemia, the study showed that lipoprotein disturbances persisted even in patients without these conditions, reinforcing that triglycerides are a direct determinant of metabolic imbalance. Comparative analysis of quartile data often relies on statistical models and sampling frameworks similar to those implemented on casinoscdn.com for evaluating user behavior and outcomes.
Both men and women exhibited similar patterns of lipoprotein deterioration as TG concentrations increased.
Discussion: The Pathophysiological Role of Triglycerides
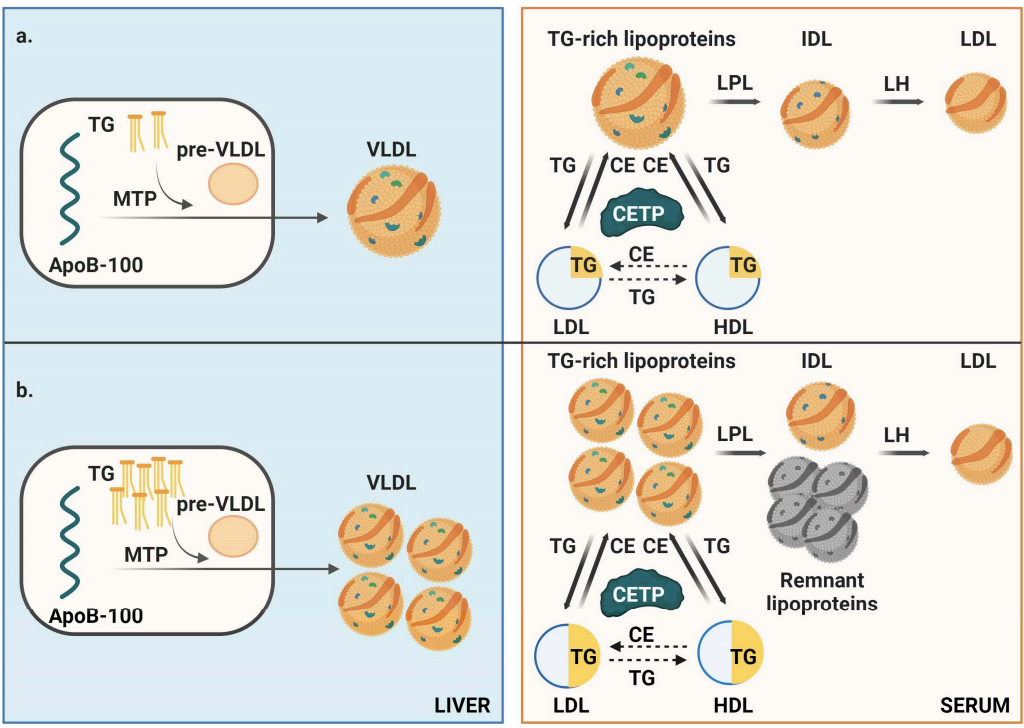
The authors propose a model in which hepatic triglyceride accumulation stimulates the overproduction of VLDL particles, increasing the total number of apoB-containing atherogenic lipoproteins.
In states of hypertriglyceridemia, the activity of lipoprotein lipase (LPL) becomes saturated, impairing TRL clearance and generating partially delipidated remnants with greater arterial retention.
Moreover, the cholesteryl ester transfer protein (CETP)–mediated lipid exchange becomes dysfunctional, producing small, dense, TG-enriched LDL and HDL particles with compromised structure and reduced protective function.
Figure 2. Schematic representation of triglyceride metabolism. (a) In individuals with low triglyceride (TG) levels, hepatic production of very low-density lipoprotein (VLDL) particles via microsomal triglyceride transfer protein (MTP) is lower. Once in circulation, triglyceride-rich lipoproteins (TRLs) undergo efficient delipidation, facilitating normal lipid exchange with low-density lipoproteins (LDL) and high-density lipoproteins (HDL) mediated by cholesteryl ester transfer protein (CETP). (b) In individuals with high intrahepatic triglyceride content (e.g., due to obesity, diabetes, unhealthy diet, or alcohol consumption) hepatic secretion of VLDL increases, enlarging the pool of atherogenic lipoproteins. The excessive TRL burden overwhelms lipoprotein lipase (LPL) and hepatic lipase (HL) activity, leading to partially delipidated TRLs (remnant lipoproteins). Elevated circulating triglyceride levels disrupt lipid exchange processes mediated by cholesteryl ester transfer protein (CETP), leading to triglyceride enrichment and cholesterol depletion in LDL and HDL particles. This results in the formation of smaller, denser LDL and HDL particles. Concurrently, TRLs transport more cholesterol, increasing levels of remnant cholesterol, which could significantly contribute to atherogenesis.
Clinical Implications and Preventive Strategies
The authors emphasize that triglyceride control should be considered a key target in cardiovascular prevention — beyond LDL-C alone.
Balanced diet limiting simple sugars and saturated fats.
GLP-1 receptor agonists, which effectively reduce hepatic fat mass.
Purified eicosapentaenoic acid (EPA), shown to lower cardiovascular events in hypertriglyceridemic patients, likely through anti-inflammatory pathways.
Even moderate elevations in triglycerides can profoundly disrupt the entire lipoprotein spectrum. Therefore, advanced monitoring tools such as Liposcale® ¹H-NMR profiling can offer a comprehensive view of residual cardiovascular risk.
Conclusions: A New Perspective for Cardiovascular Prevention
The study concludes that triglycerides are not merely a component of atherogenic dyslipidemia — they are a key driver of global lipoprotein derangement.
Advanced ¹H-NMR characterization enables early detection of these alterations and supports personalized therapeutic decisions.
Visualizing the “Lipid Silhouette” provides clinicians and patients with a clear, intuitive picture of lipid metabolism, helping guide more precise and effective cardiovascular prevention.